
Executive Summary
As pandemic-driven health, social, economic, and hunger crises deepen across the globe, it is increasingly clear that COVID-19 is widening systemic inequalities that have long affected women, girls, and other people who face discrimination because of race and migration status. These dynamics threaten decades of progress in realizing the rights and equalities that all people should enjoy, and that women have fought hard to claim. CARE has warned from the beginning that the pandemic would have a disproportionate impact on women and girls. But foresight is only as good as the action it enables. The efficacy of CARE’s and others’ COVID-19 responses depends on understanding how marginalized people are affected, in all their diversity, across contexts, and over time. Women’s needs are routinely overlooked without deliberate efforts to fill persistent gender data gaps. So we sought the advice of experts: women themselves.
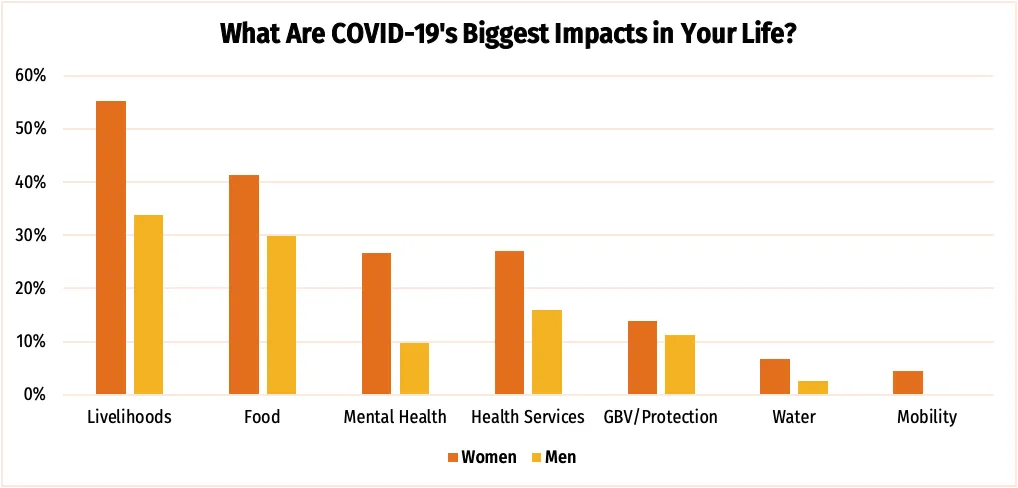
Across nearly 40 countries, the voices of more than 6,000 women bear out the dire predictions from March: that COVID-19 would result in catastrophic impacts across multiple dimensions of their lives. The growing scope of CARE’s data enables us to make more confident, global conclusions about the experiences of both women and men. Among those surveyed, women were more likely than men to report challenges across a range of areas:
- Livelihoods: 55% of the women CARE spoke to reported that income loss was one of the biggest impacts COVID-19 had for them, compared with only 34% of men. Women are more likely to work in the informal sector that COVID-19 is hitting the hardest, and have less access to unemployment benefits.
- Food security: 41% of women and 30% of men reported lack of food was a key impact COVID-19 had on their lives. This difference reflects deeply entrenched gender inequalities in local and global food systems.
- Mental health: One of the most striking differences is around mental health, where 27% of women reported this was a key impact of COVID-19—compared with only 10% of men. Women especially point to skyrocketing unpaid care burdens as a source of this stress, in addition to worries about livelihoods, food, and health care.
These findings reinforce the understanding that men and women prioritize, experience, and report on issues differently. The gaps these findings reveal illustrate the vital importance of listening to many voices, and giving diverse groups of women equal opportunity to influence people who make decisions about COVID-19 support. Only by examining these differences can we ensure that responses are designed to work effectively and reach people with the assistance they need most.
Moreover, women’s and men’s answers consistently highlight that COVID-19 responses are falling short. Inequalities are growing. Policymakers and service providers have not yet moved beyond one-size-fits-all to design COVID-19 assistance that equitably targets and supports the people who need it most. The current responses are failing to stem economic crises, hunger, and social turmoil. It is past time to move from planning to accountability. Women and other marginalized groups—especially those affected by multiple forms of discrimination—must be part of designing the COVID-19 response. Only then can the world hope to achieve any semblance of recovery.
CARE makes the following recommendations to inform a more equitable, effective COVID-19 response, and a more equal future for everyone:
- Get women and girls what they need. All actors providing support during COVID-19—either through existing safety net programs, special COVID-19 relief programs, or humanitarian aid—should focus on the areas women are prioritizing: livelihoods, food, mental health, and gender-based violence (GBV) services. Every actor must meaningfully include women in designing COVID-19 assistance. Programs should deliberately target female recipients to ensure that support effectively meets the needs of both men and women. This also means sustaining reproductive health services and GBV prevention and response as essential services.
- Invest in women leaders. COVID-19 coordination and planning platforms are most effective when they are diverse and gender-balanced. All COVID-19 leadership committees and task forces should include at least 50% women and prioritize partnering with women’s rights organizations. Actors should also work to engage men and boys in supporting women, women’s rights, and gender-equitable responses.
- Fill the data gap. This report shows the power of listening to women and girls, and how the stories they tell are different from what aggregate data shows us. It also shows that it is possible to fill the data gap to design more effective responses. All actors must collect, publish, and act on sex- and age-disaggregated data, and focus on the gaps between different people’s needs.
- Be accountable for equality. Every actor delivering COVID-19 responses should publish a status report on their activities to date and actions they have taken to listen to women’s experiences, uphold women’s rights, and ensure that women and girls have equal access to relief and recovery efforts.